30 March 2018
Dear Interested Readers,
Between “Is” and “Ought”Last week’s references and links to the ideas described in Martin Buber’s classic work
I and Thou (Ich und Du) and Desmond Tutu’s interpretation of the African concept of “Ubuntu” did not generate any comments. Despite the fact that I have no responses to suggest that my interest in those subjects is shared by readers, I am in a different space. I think that “I am in a different space” is both literally and ideologically or philosophically true. Let me explain.
First, and most obviously, I am physically in a different space. I live in a small town on the edge of the woods beside a beautiful lake between the enlightenments of Boston and Hanover. I am retired and in retreat from the day to day hassles of the work and the world in which I was once a vigorous participant. Being apart from a world that is moving fast quickly changes your perspective and may mean that what seems meaningful to me is of no interest to those who still are hard at work in the grind and in the glory of the work that is over for me.
I have moved from the role of active participant to the position of interested observer. What I see from the bleachers as I watch the ongoing game is likely to be different from the feel and the conversations down on the field of play. One of the things that once amazed me when I was on the field playing in a football game in front of 60,000 or 70,000 people was that the field was its own world and that the spectators were of little interest and seemed so far away from what I needed to be focused on in my efforts to play my role and not simultaneously sustain bodily injury.
To explain the philosophical or ideological separation that I experience when I compare what I think to what I hear and observe in much of healthcare these days I must ask for your patience as I digress to describe an insight that flowed to me in the aftermath of writing last week’s letter. Let me refresh your memory about how I introduced Buber and Tutu into the conversation. Near the end of the first section after working myself into a frenzy writing about the president’s incredibly obnoxious speech in New Hampshire on the opioid crisis, I wrote:
As I was pondering the president’s speech and trying hard to control the anger that it induced in me, I took a walk. While walking I was listening to Ezra Klein’s podcast of a recent conversation with Jaron Lanier, one of the pioneers of virtual reality and the author of several books on the interaction between humans and technology. Klein always ends his interview with the same question, “Name three books that have influenced you.” Lanier struggled with the question. His first choice was James Carse’s Finite and Infinite Games: A Vision of Life as Play and Possibility. It took Lanier several minutes of conversation to produce two more titles. I was very surprised by his second choice which really made a lot of sense in the context of what he had been saying over the last 90 minutes. His second recommendation was Martin Buber’s I and Thou. That comment hit me as the doorway to the consideration of basics of alternative approaches to so many of our current issues, including opioids and the other social concerns behind the deep divides that test us these days. When I think about Buber and I and Thou, I almost immediately think of Desmond Tutu and his focus on “Ubuntu” philosophy. It is ironic that the one reader who most frequently comments on statements like that did not get the letter. His corporate email server seems to have put me on its “blacklist.” He can’t even find the letter in “junk” and the initial attempts that I made to get the letter to him were blocked by some force beyond the technical expertise of either of us. Until Thursday it seemed like every attempt to get him the letter fell into an “IT” black hole.
My own interest in
I and Thou did take me back to Buber this week. I have the first English translation done by the
Scottish theologian Ronald Gregor Smith published in 1937. Reading any work of philosophy or theology can be as frustrating as trying to read about string theory or studying the operating manual for a complex piece of software. Buber is even more taxing, so that reading the 120 pages of
I and Thou is more of a challenge than reading the 730 pages of
Ulysses by Joyce or the 1079 pages, including endnotes, of
Infinite Jest by David Foster Wallace. [A tip for frustrated readers, try using Audiobooks to help you get over the hump.] There is a “new” (1970) translation of
I and Thou by the philosopher
Walter Kaufmann that is much better and available both on Kindle and Audiobooks. The prologue written by Kaufmann is a masterful introduction to a profound but difficult book. Kaufmann advises going slow and rereading many passages several times. I guess that is why the book seems so much longer than it is.
A few days ago I was listening to “
I and Thou” on my daily walk. I was being careful to hit the 30 second rewind as often as necessary to get as much understanding as possible out of the wisdom of Buber. One paragraph hit me “full on” like a blind sided open field block that knocks you for a flip. I got the message immediately the first time I heard it. Its wisdom became even more profound for me as I played it over and over again and then as I have read it many times. I am responsible for the bolding in the passage that captured my imagination:
It is said further that the “religious” man steps before God as one who is single, solitary, and detached insofar as he has also transcended the stage of the “ethical” man who still dwells in duty and obligation to the world. The latter is said to be still burdened with responsibility for the actions of agents because he is wholly determined by the tension between is and ought, and into the unbridgeable gap between both he throws, full of grotesquely hopeless sacrificial courage, piece upon piece of his heart.Buber, Martin. I and Thou, Trans. Kaufmann (p. 156). Kindle Edition.
On most days I do not think of myself as either a religious man or an ethical man, although on everyday the better part of me wishes that I could accept myself in the more generous and wholesome definition of either category. It is sad to imagine that “religion” has become the source of so much pain in the world that if you describe yourself as religious you are quickly into a world of “
apologetics” or dissuading others that although you hope, and have faith, that God is not dead, you are not forcing your opinion on them.
What stood out for me was Kaufmann’s translation of the last words, especially “the tension between is and ought”:
...he is wholly determined by the tension between is and ought, and into the unbridgeable gap between both he throws, full of grotesquely hopeless sacrificial courage, piece upon piece of his heart.The same passage from the Smith translation reads:
It is further said that the “religious” man stands as a single, isolated, separated being before God, since he has also gone beyond the status of of the “moral” man, who is still involved in duty and obligations to the world. The later, it is said, is still burdened with the responsibility for the action of those who act, since he is wholly defined by the tension between being and “ought to be”, and in grotesque and sacrificial courage casts his heart piece by piece into the insatiable gulf that lies between them.I like the first version better. “...tension between is and ought to be….” It just feels a little clearer than “...tension between being and ought to be…” I also like “unbridgeable gap” better than “insatiable gulf.” Buber commends the “moral” or “ethical” man but offers him little hope for success even if he throws his whole heart into his endeavors to fix what “is” that he sees “ought” to be fixed. I commend those of you who are “still involved in duty and obligations to the world. “Buber suggests that your tasks in healthcare are hard because actions required of you exceed your resources. Your labor is hard because you lack the agency you are due.
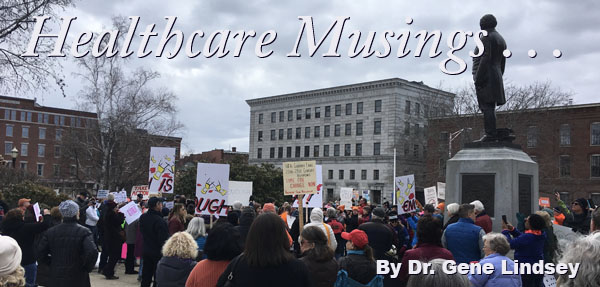
The tension between “..is and ought to be…” is Lean thinking. What “is” is imperfect and needs improvement. We call that concept “box 2” of the A3. What “ought to be” is “box 3.” I can see almost all of our concerns as tense relationships “between is and ought to be.” The picture in the header on this letter is a manifestation in the journey from “is to ought to be.” The students from Marjory Stoneman Douglas High School in Parkland, Florida led millions of people all across America including the 4000 folks that my wife and I joined in front of the state capital building in Concord. Today’s header is a picture that I took at that rally where the students demanded that we move the discussions about guns in our society from what “is” to what “ought to be.” Their effort was full of heart as they plead for relief from the adults who theoretically have the agency to end gun violence if they will just act together.
The disgust that so many people feel with the “norm” destroying behavior of the president is fueled by how far this moment “is” from where it “ought” to be in so many domains. When we realize that 10% of Americans do not have access to care we know that what “is” isn’t what it “ought” to be. The ACA has been a complicated exercise attempting to to move healthcare from where it “is” to where it “ought to be.”When we think about the poverty and structural inequality in our country we know that what “is” isn’t what “ought” to be. The difference between “is and ought” to be is the defining dichotomy of our day in almost every domain.
The challenge of “is” to “ought” to be is what Buber called the “unbridgeable gap,” or if you like the first translation, the “insatiable gap.” The combination of “is and ought” separated by a gap or gulf immediately reminds me of the 2001 call to action of Crossing the Quality Chasm. Given the fact that we have not even come close to the realization of the Triple Aim, Kaufmann’s use of “unbridgeable” seems to fit our experience better than “insatiable”, but both adjectives are consistent with the challenge that continues to confound us.
Once you are sensitized to the power of the concept of what “is” and what “ought” to be and have measured the reality of the unbridgeable gap, which we must believe is eventually bridgeable, we have a construct and language that we can use to think about more than the issues that the Marjory Stoneman Douglas students are pressing us to address. We should look at the inequities of our criminal justice system, the role of American policy in the issues of the global environment, our nation’s posture in world’s affairs, the toxic economic inequities of our society, the confusion in issues of gender, the power that men exercise over women in the workplace, and almost any issue powerful enough to appear in the comments on Twitter and Facebook. The next questions become examinations of appropriate means, the sources of intent, energy and commitment, and finally an examination of the tensions between individual concerns and the creation of an inclusive community.
Now that I have digressed to introduce the difference between “is” and “ought” and have referenced the gap that lies between them, I am able to explain why I feel more than physically separated from much of healthcare. The second sense of separation from many in healthcare and its related industries, the philosophical or ideological estrangement that I referred to before I digressed to introduce the concept of between “is” and “ought” to be, has been with me for a very long time. When I was still a very active practitioner, medical leader in group governance, and finally a healthcare executive, I was never conventional or “main stream.” I always had the sense that something about the moment was less than optimal. I believed in the work. I did not believe in the status quo. I just had a sense that we were going about it all wrong.
The concept began with the idea that it was I who was “all wrong.” Initially I felt that the estrangement was because I was a novice. I was inexperienced and therefore I felt inadequate. That made me reflective about where I was in my inadequacy, but it also made me resentful that “the powers that be” were not more effective in helping me overcome my inadequacy. It was disturbing to me that even though I was attending what was supposed to be one of the world’s best medical schools, and the feeling persisted as I moved on to being an intern, resident, and fellow in a hospital that had an international reputation, I felt as if we all were left to find our own way, or to show each other the way, while those who carried the titles that suggested they were our mentors were largely pursuing other interests.
At one point after sitting through another lecture delivered by a narcissistic academic who chose to talk about his own research rather than the basic information that I wanted to understand better, I considered making the suggestion that no professor ever be allowed to give a lecture or make a clinical presentation about a subject where they were an “authority” or had done research. The idea was that what they said was always distorted by their biases. It would be better for them to provide an outsider’s perspective on another area of medicine than their own which would force them to go through the same process of discovery that the students were going through. My idea would force them to apply their experience in a way that as I student I could not, which was to determine what was really going to be important to my patient’s care in the larger arena of the life of being a provider of care.
There was a subset of the class ahead of my class that was so upset with the quality of the teaching that they retired to the Countway Library and refused to attend lectures. They taught one another. I am told that when they took the National Boards their scores were better on average than those in their class who sat through the lectures.
When I got to the hospital I found that it was also a world where the novices were teaching one another. We learned from one another while the attendings floated in and out on the periphery and were often totally occupied with their own careers in a competitive academic environment where they were valued more for what they published, or the grants they attracted, than for the teaching they provided to us. In retrospect, I can see that in my medical school days, and as a house officer, I felt closer to and learned more from the dedicated non conformists than from those who saw their way to success through the mastery of a system that really was not working for anyone.
In the context of what I have just written it is easy for me to explain my love and respect for Robert Ebert who was paradoxically “in charge” of my medical school and should have had a reforming impact on the hospitals that I came to consider to be so dysfunctional. As I got to know him and his work after my training, I realized that we shared the same point of view. We both believed that medical education and the delivery of care were inadequate and in the need of a major overhaul. It was a situation of “is” versus “ought’ in his mind. He made the same mistakes that I reproduced over forty years later. We both failed, and I continue to fail, to make our case in a way that is adequate to cause much of a shift from “what is to what ought to be.”
If you want to know what Ebert thought about the world of healthcare fifty years ago when I was a dissatisfied student, let me suggest that you read
a speech he gave in October 1967. Dr. Ebert found more support for his transformational ideas for healthcare and medical education in Harvard Yard in Cambridge than he did in the Harvard Medical School Quadrangle in the Longwood Medical Area in Boston or at the Mass General where he had been the Physician in Chief and the Jackson Professor before he became the Dean of the Medical School in 1965. The fact that I was struggling in a system that he was leading, but knew was not what it needed to be, is just further evidence of the
...tension between is and ought, and...the unbridgeable gap between both…The Struggle to Bridge the Chasm Between the “Is” of Patient Experience and What We “Ought” to be Able to Offer EveryoneI often ask people to tell me about their healthcare. More often than my asking is the reality that as soon as someone learns that I am a retired physician I am offered their assessment of what is wrong with their care. The stories are personal and often disturbing but it is not a gross oversimplification to say that the majority of the stories could be filed under the concept of “I am treated like an ‘it’ rather than a ‘you.’”
His survival is a function of his personal resources, the amazing facility that was available to a man of his means, the constant focus on his every need by his devoted wife who patiently suffers and sifts through all of the confusion and ambiguity of the conflicting messages of his care providers who never confer with one another, and also her executive skills to manage his access to the services that he needs. She is a persistent advocate and has the focus to get him what he needs against resistance 24 hours a day, 7 days a week. Not every man is so lucky, or if your prefer, as blessed as he is.
My first response to my own story is that my family is both fortunate and blessed. My next response is that many other people in the same situation, or even in a less complicated situation, would have died long ago. After those considerations my response becomes guilt ridden from the knowledge that so many others are long gone because they were denied the resources that he is fortunate to have.
It’s complex. Much credit must be given to his personal toughness and strong will, but that would not be enough if he did not have much more than adequate personal resources, a dedicated caregiver, and access to a system that gives him much more than he really needs most of the time, even as it fails to give him what he really needs some of the time.
It is ironic that despite the fact that he still lives, a very frequent conversation that my sibs and I have is whether or not we should suggest to his wife that they change several of his providers. It seems that he lives because the system provides what he needs by providing too much in ways that both sustain him and exhaust him and his wife. There is no doubt that what “is” is not what “ought” to be and establishing what “ought” to be is far beyond our ability to help. It is impossible to make a system that is inefficient and difficult to use work better for just one individual. Systems of care are so complex that they must be improved for populations, for everyone every time, or they will be reliable for no one anytime.
Perhaps I should not focus on the hundreds of thousand of dollars of cost and the hours and hours of avoidable tedium that has sustained my father because he is alive. I should be delighted that he is hanging on to be around to see his four children and their spouses, and his twelve grandchildren and their spouses, and his thirteen great grandchildren with no spouses yet, at the family gathering scheduled for June. The gap between what “is” and what “ought” to be is greater for many others than for him, and there is no equity in that fact.
Bad systems are not discriminatory. They threaten everyone. Sure, those that have no access to any care are the ones who stand in greatest need, but cynical house officers have long known that the ultra luxurious hospital rooms reserved for the very rich in some of our most impressive institutions are often so gated from the hoi polloi that their barriers can create a distance from the care that the denizens of those luxurious surroundings really need. Was the president really served well when his physician told him that he was very healthy and had nothing in the moment or in the future to cloud the prospects for a long life? The very powerful and the very privileged suffer other people’s inability to be objective about them. The ultra privileged carry the unusual burden of too much care.
I have observed that the importance of what “is” and “ought” to be varies across all six domains of quality: patient centeredness, safety, timeliness, efficiency, effectiveness, and equity. Some would say the prime concern is safety, and they might be right. Others are concerned most with cost and value as manifested by variations in efficiency, effectiveness, and timeliness. I respect their opinions and understand that cost and the aligned concept of value are an enormous challenge across all populations. But, I believe the hardest to achieve components of the six domains of quality, the ones for which the chasm between what “is” and what “ought” to be is greatest, are equity and then patient centeredness. Our ability to relate to our patients as a true “you” in dialogue and reciprocity with our medical “I” is a dramatic example of the gulf between “is” and what “ought” to be.
I believe our ability to cross the chasm from “is” to “ought” is more than a systems issue, but I also believe that the “noise” from our systems issues, and all the other issues that compete with healthcare for the attention of our leaders and the public, make the gap between “is” and “ought” much wider. The dysfunction in our systems generates burnout for our medical professionals and frustration for our patients. We can not build the bridges from “is” to “ought” without focusing on how dysfunctional systems widen our gaps and make it harder to engage all people, as “you.” But above all, we must see everyone, those with access and resources and those denied access and bereft of resources, as “you.”
Dr. Martin Luther King, Jr. was the greatest advocate of our age for treating everyone as a “you” and breaking down the barriers to equity that have existed as far back into antiquity as we can see. He paid the ultimate price that is associated with efforts to lead us from “is” to “ought.” This coming Wednesday will be the fiftieth anniversary of Dr. King’s assassination. There can be much debate about how far we have moved “is” toward “ought” since Dr. King fell before a sniper’s bullet on April 4, 1968. I will say more in next week’s letter, but I hope that you will pause next Wednesday, as I will, to focus on his message and remember him if you can, or if you only know him from history, that you will spend some time this week expanding your knowledge of him and all of his efforts to move us from what “is” to what “ought” to be.
Let’s Play Ball! The Ephemeral Joys of Opening Day
If your focus is religion, this week is a busy one with Passover and Easter. If your focus is mostly in this world and on sports then you have the Final Four Weekend to savor after baseball’s Opening Day. I typed much of this letter while watching the Red Sox start their march toward the World Series with their opener in St. Petersburg against the Tampa Bay Rays. The joy of Opening Day was short lived. The bottom of the eighth inning was a disaster as the Sox bullpen blew a 4-0 lead giving up six runs on plenty of walks and hits. It was hard to take. Now I am looking forward to the home opener next Thursday. We will be there in our parkas.
Today, Good Friday, I will play Saint Peter in the noontime ecumenical service in our little town. The role is pretty easy. I just hang around the periphery of things and say “I am not” every time someone asks me if I am a disciple. Then I get upset when the cock crows. Friday night there is a seder, and then comes Easter Sunday.
Perhaps religion and the secular life will come together if
Loyola of Chicago is prayed into the championship game of the NCAA tournament against Villanova by their
98 year old mascot nun, Sister Jean. Loyola of Chicago is a Jesuit Institution.
Villanova was founded by the Order of Saint Augustine. So, it would be the Augustinians versus the Jesuits. How Sister Jean’s prayers might play out in such a complicated circumstance is beyond my understanding of theology. Perhaps, with or without God’s attention to Sister Jean’s prayers, the best resolution might be that Villanova loses to Kansas and Loyola loses to Michigan in the semifinals so that we can then keep the spiritual and the mundane worlds separated. Whatever happens, March Madness has lived up to its name and its billing. The unexpected has already occurred.
Whatever your plans for the weekend I hope that you will be renewed. There is much too do and much energy will be required if we are ever to move so many concerns from what “is” to what “ought” to be.